Why do some Candida infections keep returning even after treatment? The answer often lies in the biofilm’s tough armour that protects yeast cells from drugs, immune responses, and environmental stress.
Vaginal Candida infections affect 3 in 4 women at least once in their lifetimes. In India, vulvovaginal candidiasis accounts for an estimated 25 – 60% of symptomatic vaginal discharge cases, though prevalence varies by region and study population. Their significant treatment barriers are the development of dense microbial layers ‘biofilms’, which contribute to antimicrobial resistance and infection recurrence.
Understanding the challenge
(This section explains why biofilms are such a formidable barrier and why new therapeutic strategies are urgently needed).
Candida albicans (C. albicans) is a dual-natured pathogen, commensal under normal conditions yet opportunistic when the vaginal environment shifts. Even small disturbances in the natural acidic pH can allow Candida to overgrow. Its partner in crime is biofilm formation, a protective layer that acts like a bodyguard for fungal cells, shielding them from antifungal drugs, immune defences, and everyday stressors. This process is why many women continue to experience repeated infections even after completing treatment.
As highlighted in our earlier work, vaginal Candida infections remain one of the most common reproductive tract infections worldwide, yet biofilm-associated cases are often underdiagnosed and undertreated.
Biofilms are not just passive barriers; they are dynamic microbial ecosystems that mature, disperse, and seed new infections, as research has shown.
This challenge shaped my PhD research question: could we design a novel, drug-loaded vaginal nanogel that targets both fungal cells and their biofilms?
Why a new drug? Because many existing antifungals struggle once Candida settles into a biofilm.
Why a gel? Because it adheres well to the vaginal cavity and remains in place long enough to exert its therapeutic effect.
Why nanoscale? Because tiny particles can penetrate deeper into vaginal tissues and deliver higher drug concentrations directly to the infection site.
Formulation mission: Research techniques
(The following section outlines the scientific approaches used to identify, test, and refine this nanogel formulation).
To identify the right drug candidate, we used computer-aided screening approaches to compare several candidates with existing antifungals. Luliconazole stood out for its anti-microbial activity against C. albicans, making it the most promising choice for our nanogel. In laboratory (in vitro) and animal (in vivo) studies, both luliconazole and the nanogel showed a favourable skin profile, Candida inhibition, and the ability to disrupt dense biofilms.
However, choosing the right drug was only half the challenge; the formulation itself had to be compatible with the biology of the vaginal environment. To address this, we developed a luliconazole‑loaded nanogel specifically designed for vaginal application. The gel was engineered to stick to the mucosal surface, release the drug slowly over time, and penetrate deeper tissue layers where biofilms persist.
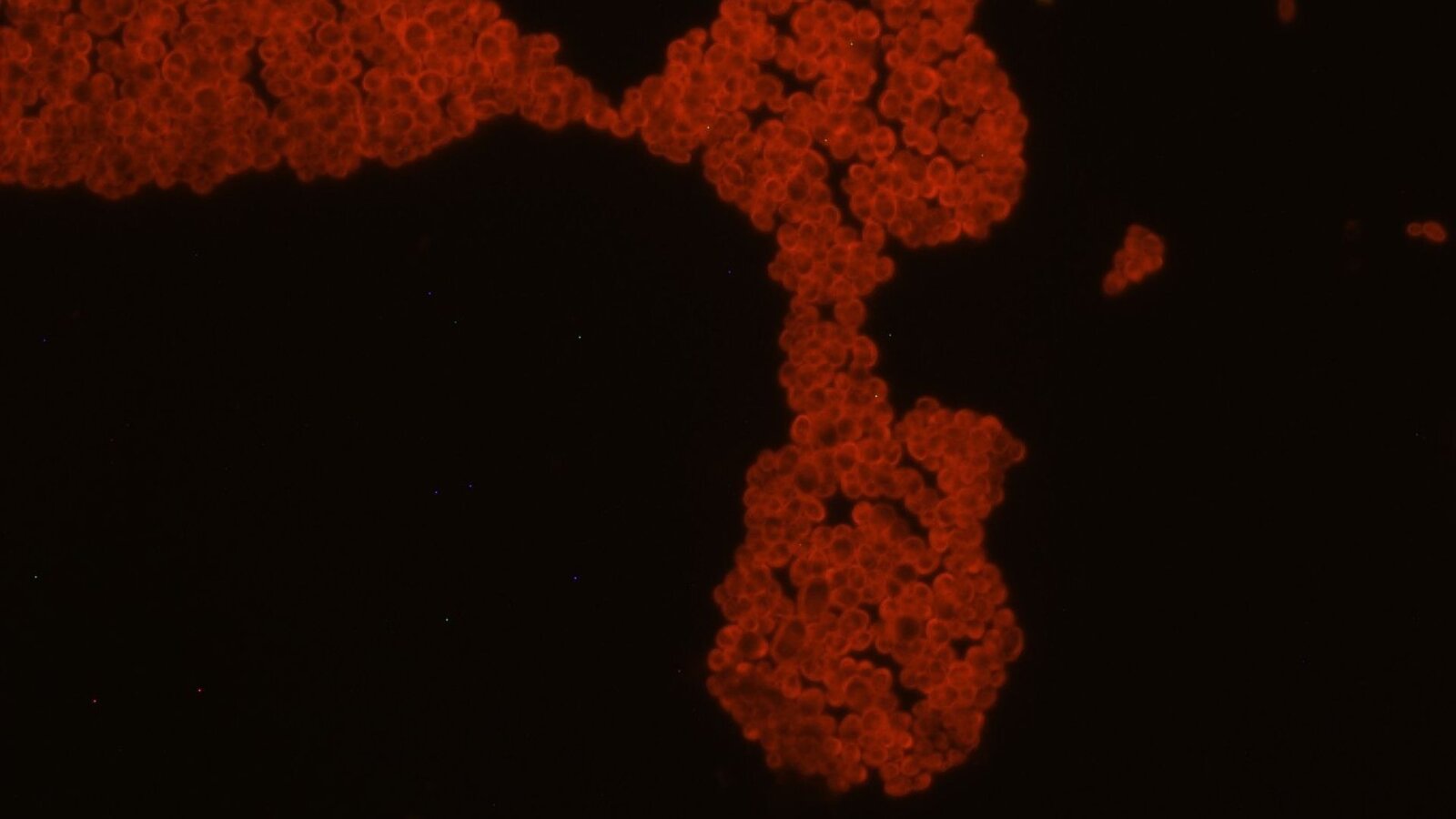
When tested on clinical isolates from symptomatic patients, the nanogel significantly inhibited fungal growth and disrupted the architecture of mature biofilms. The biofilms were visualised by fluorescence microscopy, revealing fragmented layers and not clusters. Skin-safety tests using goat vaginal tissue further confirmed that the nanogel was non-irritant when applied locally.
Research relevance: Luliconazole, reimagined for biofilms
(This section highlights the research novelty uncovered in our work).
For the first time, luliconazole showed dual activity against C. albicans clinical isolates, both inhibiting fungal growth and disrupting established biofilm structures. Using clinical isolates from patients, we captured real-world disease behaviour, revealing previously unreported antibiofilm activity of luliconazole when delivered via a vaginal nanogel system.
To assess drug performance, we measured the minimum concentrations required to inhibit C. albicans growth, prevent biofilm development, and reduce established biofilms. In all cases, luliconazole achieved these effects at lower concentrations than standard antifungal therapy, reinforcing its selection as the lead drug for our proposed nanogel.
Translational impact
(This section highlights how the nanogel could translate into a practical therapeutic option for vaginal Candida infections)
This work bridges a critical gap in vaginal antifungal therapy. The combination of luliconazole with a nano-lipid gel offers a locally acting, easy-to-apply, and potentially cost-effective formulation strategy. The designed nanogel provides a tailored approach to disrupt C. albicans biofilms and improve therapeutic outcomes.
The formulation holds promise for clinical translation, particularly in settings where vaginal Candida infections are underdiagnosed and undertreated. Future studies may explore advanced delivery platforms for both acute and chronic vaginal Candida infections, thereby strengthening the translational pipeline for innovations in women’s healthcare.